AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2640-1053/081
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Manchester, M8 5RB, United Kingdom.
Citation: Anthony Kodzo-Grey Venyo. (2021) Signet-Ring Cell Carcinoma of the Urinary Bladder: A Review and Update. Cancer Research and Cellular Therapeutics. 5(2); Doi: 10.31579/2640-1053/081
Copyright: © 2021, Anthony Kodzo-Grey Venyo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 April 2021 | Accepted: 05 May 2021 | Published: 07 May 2021
Keywords: Signet-ring cell carcinoma; adenocarcinoma; urinary bladder; primary; metastatic; stomach; colon; histopathology; CT scan; esophagogastroduodenoscopy; colonoscopy; biopsy; radical cystectomy; chemotherapy; radiotherapy
Signet-ring cell carcinoma of the urinary bladder is an uncommon histopathology variant of carcinoma of urinary bladder which has been stated to account for 0.5% and 2% of primary malignant tumours of the urinary bladder. Signet-ring cell carcinoma of the urinary bladder is stated to either arise from the wall of the urinary bladder or from remnants of the urachus, or signet-ring cell carcinoma of the urinary bladder could also develop as a metastatic tumour that has ensued a primary signet-ring cell carcinoma that had arisen from a number sites of the body some of which include: the stomach, colon, or breast, the appendix and other organs. It has been iterated that the least common type of signet-ring cell carcinoma is primary signet-ring cell carcinoma and that up to 2013 less than 100 cases had been reported. Signet-ring cell carcinoma of the urinary bladder can affect males as well as females, young individuals or adults. Signet-ring cell carcinoma of the urinary bladder could be diagnosed incidentally or it may present with non-specific symptoms that simulate the symptoms of other urinary bladder tumours including: lower urinary tract symptoms, haematuria, abdominal pain / discomfort or loin pain, retention of urine, feeling unwell, or weight loss. Microscopy examination of the tumour whether it was obtained by means of trans-urethral resection or by cystectomy would tend to demonstrate a tumour that is comprised of signet-ring cells that contain peripherally pushed hyperchromatic nuclei, intra-cytoplasmic mucin, as well as lakes of extracellular mucin. The tumour cells could be arranged in lobules, and separated by fibrovascular septae. There tends to be visualization of mitosis as well as evidence of necrosis. The tumour tends to be seen within the underlying stroma and quite often within the detrusor muscle and up to the extra-vesical fat quite often. Immunohistochemistry staining studies of signet-ring cell carcinoma of the urinary bladder would tend to show tumour cells that exhibit positive staining for: Cytokeratin including cytokeratin 7, CAM 5.2, AE1/3, and 34ßE12; Vimentin; Peanut lectin agglutinin; Ulex europaeus agglutinin. In signet ring cell carcinoma of urinary bladder immunohistochemistry staining of the tumour may also show tumour cells that exhibit positive staining for the following tumour markers: CK, CK7, CK20; CDX2; Villin - There could be a small amount of positive staining for Villin. In signet-ring cell carcinoma of the urinary bladder, immunohistochemistry studies of the tumour may demonstrate tumour cells that do exhibit negative staining for the ensuing tumour markers: Vimentin, (this does show therefore that some tumours would stain positive and others would stain negative); GATA3, and P53. To confirm whether a signet-ring cell carcinoma of the urinary bladder is a pure primary tumour or metastatic tumour does require detailed history taking with evidence of previously treated signet-ring cell carcinoma elsewhere and comparing the pathology features of the tumours, the undertaking of radiology imaging including ultrasound scan, computed tomography scan or magnetic resonance imaging scan of abdomen and pelvis as well as upper gastrointestinal endoscopy and lower gastrointestinal endoscopy to ascertain if there are any lesions within the gastrointestinal tract and taking biopsies of any suspicious lesion found for pathology examination and comparing the features of the lesions with the urinary tract tumours. There is no consensus opinion of the treatment of signet-ring cell carcinomas of the urinary bladder even though it has been realised that primary signet ring cell carcinomas have tended to be more invasive and higher staged as well as associated with very poor prognosis in comparison with the traditional urothelial carcinoma. Treatment options that have been utilized have included: trans-urethral resection of tumour, radical cystectomy alone or radical cystectomy plus adjuvant therapy and despite utilization of radical cystectomy and adjuvant therapy majority of patients tend to die. There are sporadic reports of isolated cases of good short-term, medium-term, and long-term survival usually if the tumour is diagnosed at an early stage. Early diagnosis, aggressive complete surgical excision of primary and metastatic signet-ring cell carcinomas and utilization appropriate combination adjuvant therapies would provide the best treatment of curative intent. Additionally, there is an anecdotal report of an effective treatment of an advanced metastatic primary signet-ring cell carcinoma of the urinary bladder with utilization of docetaxel which resulted in destruction of the tumour cells without an operation which would indicate that some chemotherapy agents could be good enough for the successful treatment of signet-ring cell carcinomas of the bladder including primary and metastatic tumours. Therefore, it is possible that novel treatment options of treatment of signet-ring cell carcinoma of the urinary bladder including an appropriate chemotherapy plus additional non-operative treatments including cryotherapy, radiotherapy, radiofrequency ablation, irreversible electroporation, selective angiography and chemical infusion of chemotherapy agents into the tumour plus immunotherapy could be explored as treatment options. There is a global need for urologists, oncologists, and pharmacotherapy research workers to identify new chemotherapy medicaments that would safely and effectively destroy primary and metastatic signet-ring cell tumours in order to improve upon the outcome of the disease. A global multi-centre trial of various aggressive treatment options should be commenced quickly.
Signet-ring cell carcinoma of the urinary bladder is an uncommon histopathology variant of adenocarcinoma of the urinary bladder that tends to be characterised by the production of mucus and presence of signet-ring appearance of the tumour cells on histopathology examination of the tumours in which the nuclei of the tumour cells are pushed to the periphery of the tumour cells. Signet-ring cell carcinoma of the urinary bladder can be a primary signet-ring cell carcinoma of the urinary bladder or a metastatic signet-ring cell carcinoma with the primary signet-ring cell carcinoma originating elsewhere. With regard to metastatic signet-ring cell carcinoma of the urinary bladder, the primary tumour may have previously been treated with the metastatic urinary bladder signet-ring cell carcinoma subsequently developing, or at times the primary tumour may be contemporaneously diagnosed when the metastatic signet-ring cell carcinoma of the urinary bladder initially manifests in association with symptoms of the primary tumour or the primary tumour could be diagnosed following detailed investigations undertaken by the urologists including radiology imaging and upper and lower gastrointestinal endoscopy procedures and biopsies of lesions found during these investigations. Primary Signet ring-cell carcinoma (SRCC) of the urinary bladder is said to be a relatively uncommon subtype of adenocarcinoma which has stated been to comprise only of 0.5% to 2% of primary carcinomas of the urinary bladder [1]. Following the first case of primary signet-ring cell carcinoma of urinary bladder which had been reported in 1955 by Saphir, [2,3] sporadic cases, case series and studies on primary and metastatic signet-ring cell carcinomas of the urinary bladder have been reported in the global literature. But because of the rarity of primary and metastatic signet-ring cell carcinomas of the urinary bladder, it would be envisaged that majority of clinicians including general practitioners, urologists, and pathologists, as well as oncologists would not have encountered a case of the disease before and hence they might not be familiar with the diagnostic features, biological behaviour, management, and management outcome of the tumour. Primary signet-ring cell carcinoma of the urinary bladder does have similar histopathology examination characteristics as that of primary signet-ring cell carcinomas of the gastrointestinal tract, breast, lung, gall bladder, prostate gland, and other organs and hence further evaluations to ascertain the primary sites of these tumours have been stated to be mandatory [3]. Considering that signet-ring cell carcinoma of the urinary bladder, whether it is a primary or metastatic tumour is an uncommon tumour, it would important for clinicians to have an overview background knowledge of signet-ring cell carcinomas generally and then about signet-ring cell carcinomas of the urinary bladder in order to be up to date with the diagnosis and management of signet-ring cell carcinomas of the urinary bladder whether primary or metastatic. The ensuing article has been divided into two parts: (A) Overview which has discussed various general aspects of signet-ring cell carcinomas affecting other organs and the urinary bladder and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to signet-ring cell carcinoma of the urinary bladder.
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Signet-ring cell carcinoma; Signet-ring cell carcinoma of bladder; primary signet-ring cell carcinoma of urinary bladder; metastatic signet-ring cell carcinoma of the urinary bladder; signet-ring cell carcinoma metastatic to the bladder. Forty eight references were identified which were used to write the article that has been divided into two parts: (A) Overview which has discussed various general aspects of signet-ring cell carcinomas affecting other organs and the urinary bladder and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to signet-ring cell carcinoma of the urinary bladder.
[A] Overview
General Overview of signet-ring cell carcinomas with emphasis on general overview of signet-ring cell carcinoma of the urinary bladder with miscellaneous discussions of signet-ring cell carcinomas of other organs.
Definition and General Statements
The presentations of signet-ring cell carcinomas of the urinary bladder could include:
(a) An incidental finding.
(b) loin/flank/back/abdominal pain or discomfort
(c) Weight loss / loss of appetite
(d) Feeling unwell
(e) Other nonspecific symptoms
(f) Lower urinary tract symptoms
(g) Haematuria.
(h) Retention of urine.
Some of the possible clinical examination findings in cases of signet-ring cell carcinomas of the urinary bladder could include:
(a) No abnormality within the abdomen.
(b) Tenderness in the loin.
(c) suprapubic tenderness and occasionally a palpable suprapubic urinary bladder mass.
(d) If associated contemporaneously with signet-ring cell carcinoma elsewhere like the gastrointestinal tract some of the symptoms could include: nausea, vomiting, diarrhoea, abdominal distention.
(e) In cases of a previous surgical excision of a signet-ring cell carcinoma of the gastro-intestinal tract or any abdominal organ, there would be a surgical scar in the abdomen
Laboratory Investigations
Urine
Haematology blood tests
Biochemistry Blood tests
Chest X-ray
Ultrasound scan
Computed Tomography (CT) scan
Magnetic Resonance Imaging (MRI) Scan
Positron Emission Tomography / Computed Tomography Scan
Isotope Bone Scan
Upper Gastrointestinal Endoscopy
In order to confirm whether or not a signet-ring cell carcinoma of the urinary bladder is a primary tumour or metastatic tumour from the gastro-intestinal tract, upper gastrointestinal endoscopy and lower gastrointestinal endoscopy plus biopsy of tumours or suspicious areas of the stomach and lower bowel tend to taken for pathology examination and the features of the lesions of the urinary bladder tend to be compared with the features of biopsies obtained from the gastrointestinal tract. If an individual has previously had surgery for any previous signet-ring cell carcinoma excised from the stomach or the bowel, the old specimens always tend to be reviewed and compared with the specimens that have been obtained from the urinary bladder.
Colonoscopy
In order to confirm whether or not a signet-ring cell carcinoma of the urinary bladder is a primary tumour or metastatic tumour from the gastro-intestinal tract, upper gastrointestinal endoscopy and lower gastrointestinal endoscopy plus biopsy of tumours or suspicious areas of the stomach and lower bowel tend to taken for pathology examination and the features of the lesions of the kidney / renal pelvis / upper urinary tract tend to be compared with the features of biopsies obtained from the gastrointestinal tract. If an individual has previously had surgery for any previous signet-ring cell carcinoma excised from the stomach or the bowel, the old specimens always tend to be reviewed and compared with the specimens that have been obtained from the kidney / renal pelvis / upper urinary tract.
Treatment
Treatment of signet ring cell carcinomas of the urinary bladder could include the following options:
Macroscopy examination features
Macroscopy examination of a cystectomy specimen in cases of signet-ring cell carcinoma of the urinary could demonstrate a well-circumscribed, firm, tumour which could occupy any part of the urinary bladder that has been involved by the tumour. The cut surface of the tumour would tend to be found to be whitish-yellow and it may be associated with focal areas of haemorrhage as well as macro-cysts. Normal urinary bladder tissue could be observed in other parts of the urinary bladder that is not involved by the tumour. The tumour may be found to be confined to the bladder in some cases but if it can also be found to have extended to or beyond the peri-vesical fat. This would be observed but the features would be non-specific and not diagnostic of the tumour therefore microscopy examination features and the immunohistochemistry staining features of the tumour are always needed to confirm the diagnosis.
Microscopy examination features.
Depending upon whether a signet-ring cell carcinoma of the urinary bladder is a pure or mixed signet-ring cell carcinoma, various microscopy examination features would be seen including: Signet-ring cell tumour cells only or signet-ring tumour cells plus other types of tumour cells including adenocarcinoma, urothelial carcinoma (transitional cell carcinoma) plus signet-ring cell tumour cells, tumour cells that contain intracellular mucin-filled vacuole displacing hyperchromatic nucleus to one side which would be indicative of signeting cell carcinoma.
Immunohistochemistry
Positive staining
In signet-ring cell carcinoma of the urinary bladder, tract, immunohistochemistry staining studies of the tumour does demonstrate tumour cells that exhibit positive staining for the following: [26]
In signet ring cell carcinoma of urinary bladder immunohistochemistry staining of the tumour may also show tumour cells that exhibit positive staining for the following tumour markers:
Negative staining
In signet-ring cell carcinoma of the urinary bladder, immunohistochemistry studies of the tumour may demonstrate tumour cells that do exhibit negative staining for the following tumour markers:
Electron Microscopy examination features
Differential Diagnoses
Some of the differential diagnoses of primary / secondary signet-ring cell carcinoma of the urinary bladder include:
Prognosis / Outcome of signet ring cell carcinomas affecting different organs
Outcome
With regard to the prognosis based upon the organ of the body affected by signet-ring cell carcinoma, it has been iterated that on the whole signet-ring cell carcinomas had tended to be aggressive tumours that had tended to be diagnosed at advances stages of the disease and survival of patients who have been afflicted by signet-ring cell carcinoma has generally tended to be shorter in comparison with other non-sigmoid cell carcinomas of the various organs. It has been iterated that the outcome of signet-ring cell carcinoma as well as its chemosensitivity with utilization of specific treatment regimens in majority of studies have remained controversial in view of the fact that its poor prognosis could be related to its more advanced stage at the time of diagnosis [14].
Some authors had suggested in their study that the dismal prognosis of signet-ring cell carcinoma would seem to be caused by its intrinsic tumour biology which should constitute a basis for further new research on signet-ring cell carcinomas [22].
Urinary bladder
Stomach signet-ring cell carcinoma.
Kidney, renal pelvis, and upper urinary tract.
Prognosis and staining for vimentin
It is worth pointing out that positive staining for vimentin would not be diagnostic of signet-ring cell carcinomas but that it has been pointed out that the prognosis of patients who had vimentin positive gastric carcinomas was significantly (P < 0.001) worse than the prognosis of patients who had vimentin negative gastric carcinomas. They iterated that the expression of vimentin in gastric cancer might contribute to the high invasive phenotype of gastric cancer and could represent a useful biological marker to determine the biological aggressiveness of gastric carcinoma [31].
By extrapolation, it is likely that signet-ring cell carcinomas of the kidneys, renal pelvis, and upper urinary tract that exhibit positive immunohistochemistry staining for vimentin could turn out to be more invasive tumours and tumours that portend a more aggressive type of tumour in comparison with signet-ring cell carcinomas of the kidney, renal pelvis, and upper urinary tract that exhibit negative staining for vimentin but this would need to be confirmed by the inclusion of immunohistochemistry staining for vimentin in a global multi-centre clinical study on signet ring cell carcinomas of the kidney, renal pelvis, and upper urinary tract.
In another study of signet ring cell carcinoma of the upper urinary tract immunohistochemistry staining of the tumour showed tumour cells that exhibited positive staining for the following tumour markers: [32] CK, CK7, CK20. CDX2, Villin. There was a small amount of positive staining for Villin. The study also reported negative staining for the following: [32] Vimentin, (this does show therefore in comparison with above some tumours would stain positive and others would stain negative), GATA3, and p53.
[B] Miscellaneous narrations and discussions from some case reports, case series, and studies related to signet-ring cell carcinoma of the urinary bladder.
Boukettaya et al [33]. Reported two cases of signet-ring cell carcinoma as follows:
Case 1
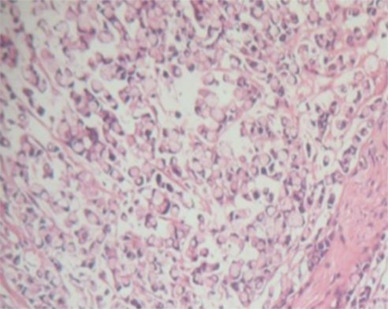
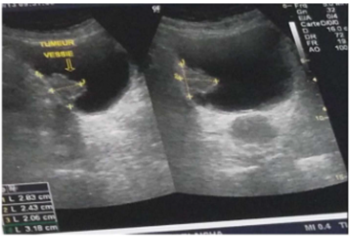
A 72-year-old man had presented with intermittent painless, total, visible haematuria, urinary urgency, and pollakiuria. He did not have any significant past medical and family history. His general and systematic as well as abdominal examinations were normal. He had ultrasound scan of abdomen and pelvis and renal tract which demonstrated bilateral hydroureteronephrosis and thickening of the wall of the urinary bladder. He had cystoscopy which demonstrated a solid mass within the left side wall of his urinary bladder which was biopsied and histopathology examination of the biopsy specimen showed a proliferation of round-cell aspect of signet-ring. Immunohistochemistry staining of the specimen demonstrated positive immunohistochemistry staining for cytokeratin 7 and negative staining for cytokeratin 20. A diagnosis of signet-ring cell adenocarcinoma of the urinary bladder was made. He had computed tomography (CT) scan of abdomen and pelvis, which did not demonstrate any locoregional lymph nodes, metastases, or a primary tumour within any abdominal or pelvic organ. He underwent gastrointestinal endoscopy assessments and these did not demonstrate any primary tumour within the gastrointestinal tract. A diagnosis of primary signet-ring cell carcinoma of the urinary bladder was made. He underwent radical cystoprostatectomy. Histopathology examination of the tumour demonstrated features of a signet-ring cell adenocarcinoma that contained a colloid component which was estimated to be about 40%. The tumour was reported as invasive and it had extended into the peri-vesical fat together with evidence of the tumour within the lymphatics as well as nerve sheathing (see figure 1). The surgical resection margins of the tumour were noted to be free of tumour. The tumour was staged as PT3N0M). He did not receive any adjuvant treatment. He re-presented 16 months subsequently with haematuria as well as perineal pain. He had urethroscopy which demonstrated stenosis within his anterior urethra and the site was biopsied and pathology examination showed features that confirmed the diagnosis of recurrence of signet-ring cell carcinoma within the urethra. He underwent radiotherapy to the tumour and the urinary bladder area (pelvis). He underwent clinical and radiology imaging follow-up assessments every 6 months during which he had computed tomography can of his thorax, abdomen, and pelvis. At his 3-years follow-up assessment, he had continued to have a good quality of life as well as radiology image stability.
Case 2
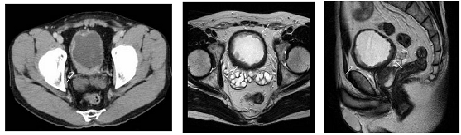
A 64-year-old man who did not have any significant past medical history had presented with a 2-month history of total visible haematuria. He had ultrasound scan of renal tract and pelvis which demonstrated an infiltrating mass within the posterolateral wall of his urinary bladder as well as left hydroureteronephrosis. He underwent cystoscopy which revealed a polypoid mass upon the left posterior-lateral urinary bladder. Trans-urethral resection of the urinary bladder tumour (TURBT) was undertaken. Pathology examination of the urinary bladder tumour chips demonstrated features of a poorly differentiated invasive signet-ring cell carcinoma of the urinary bladder. He had computed tomography scan of abdomen which demonstrated a large effusion which had occupied his entire abdomen and as well as peritoneal cavity with no CT scan evidence of peritoneal carcinomatosis. He underwent gastroduodenoscopy and colonoscopy which did not demonstrate presence of any suspicious lesion. The evolution of the disease process was marked by the development of ascites. Aspirate of the peritoneal fluid was examined by cytology assessment and this confirmed presence of neoplastic cells (see figure 2). Palliative chemotherapy was discussed but this could not be administered in view of his deterioration and he died 5 months pursuant to the diagnosis of his malignant tumour.

Akamatsu et al. [34] undertook a comprehensive review and analysis of the clinical characteristic of primary signet-ring cell carcinoma of the urinary bladder cases that had been reported within Japan. They reviewed all articles that had been reported from Japanese institutions regardless of their language. Overall they had identified 131 titles that had been reported between 1981 and 2008. They excluded meeting abstracts, but the unpublished cases within their institution were included. In all they comprehensively reviewed 54 cases and analysed them. Akamatsu et al. [34] summated their results as follows:
Akamatsu et al. [34] made the following conclusions:
Considering that Akamatsu et al. [34] had found out that the prognosis of high-staged IV primary signet-ring cell carcinomas is poor, it would be argued that academic oncologists, urologists, and pharmacotherapy research workers should endeavour to find new chemotherapy medications that would effectively and safely destroy primary signet-ring cell tumours of the urinary bladder in order to improve upon the survival and quality of life of the patients.
Bouhajja et al. [35] reported two patients who were aged 53 years in the case of a man, and 70 years in the case of a woman. They manifested with right back pain, burning upon micturition, and visible haematuria. They had ultrasound scan of abdomen, which demonstrated a thickened urinary bladder wall that measured 8 mm with regard to thickness. The ultrasound scan did reveal a budding intravesical lesion with a calculation of the left lower ureter that measured 5 mm in its greatest diameter. They underwent cystoscopy which demonstrated an atypical tissular lesion that that was frayed whitish and solid upon the cut surface. The woman had magnetic resonance imaging (MRI) scan of the pelvis which demonstrated a cervix ill-limited tissue mass that had invaded her anterior vaginal wall. Trans-urethral resection of the urinary bladder tumour (TURBT) was undertaken with regard to one case, and a biopsy of the urinary bladder lesion was undertaken in the other case. Immunohistochemistry staining study of tumours showed that tumour cells of both tumours had exhibited positive staining for CK7. Based upon the features of the tumours, a diagnosis of signet-ring cell carcinoma of the urinary bladder was made in each case. Bouhajjia et al. [35] made the following conclusions:
Additionally, it would be argued that since it is known that muscle invasive signet-ring cell carcinomas of the urinary bladder tend to be associated with aggressive biological behaviour and poor prognosis ensuing in death, it would be important to treat such tumours aggressively and that a global multi-centre trial of various treatments including (a) radical cystectomy plus (b) adjuvant radiotherapy, plus (c) adjuvant combination chemotherapy, plus immunotherapy should be considered in all cases.
Hamakawa et al. [36] reported a53-year-old Japanese man, who presented with pain on voiding as well as visible haematuria for many months. He did not have any significant past medical history and he was treated with a course of antibiotics for a presumed urethritis which did not resolve his symptoms. He had urinalysis which showed red blood cells 50-99 / high power fields, and white blood cell count of 10 to 19 per high power field but there was no growth of bacteria in his urine, as well as his urine cytology was negative. The results of his serum tumour markers that included carcinoembryonic antigen were all within normal limits. He underwent cystoscopy which demonstrated widely prevalent non-papillary raised lesions as well as oedematous mucosa upon the posterior wall of the urinary bladder. He had computed tomography (CT) scan of pelvis which showed marked diffuse thickening of the wall of his urinary bladder with no evidence of pelvic lymph node enlargement. He also had magnetic resonance imaging (MRI) scan which showed results that were similar to the results of his CT scan. Furthermore, sagittal MRI scan demonstrated thickening of the wall of his urinary bladder from the anterior wall to the posterior wall of the urinary bladder (see figure 3). Trans-urethral resection biopsy was undertaken and histopathology microscopy examination of the biopsy specimen showed signet-ring cell carcinoma with poorly differentiated adenocarcinoma. He next underwent gastroscopy, colonoscopy as well as radionuclide scanning in order to exclude an extra-vesical primary site of the tumour. Based upon the negative findings of the gastroscopy, colonoscopy and the radionuclide scanning a final diagnosis of signet-ring cell carcinoma of urinary bladder (SRCCU) was made. He underwent radical cystectomy with pelvic lymph node dissection and ileal neo-bladder construction. Macroscopy examination of the excised specimen demonstrated diffuse thickening of the wall of the urinary bladder and oedematous mucosa of the urinary bladder with reddened as well as erosive areas. Microscopy histopathology examination of the specimen demonstrated diffuse infiltration of tumour cells, abundant formation of mucin, with positive staining for periodic acid-Schiff, resulting in compression of the nucleus, which is a typifying feature of signet-ring cell tumour that had invaded the layer of a serous membrane as well as vessel invasion which was reported as a high-grade, pT3bN0M0 v(+) tumour (see figure 4). He received adjuvant combination chemotherapy with S-1 and cisplatin. He did receive S-1 (80mg/m2, on days 1 to 14, and cisplatin 70 mg /m2 on day 8 for 3 cycles. He has continued to be well and he was alive at his 90 months post-operative follow-up assessment with no evidence of local tumour recurrence or metastasis.
This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Wang et al. [37] undertook a study to directly compare the cancer-specific survival of patients who had signet-ring cell carcinoma (SRCC) of the urinary bladder with patients who had urothelial carcinoma (UC) of the urinary bladder. Wang et al. [37] identified patients who had a diagnosis of SRCC of the urinary bladder and urothelial carcinoma (UC) of the urinary bladder, in the Surveillance, epidemiology, and end results programme (SEER) (2001-2004). They compared the demography of the patients and the clinical characteristics of the patients at the time of their initial diagnosis. They compared the differences in the cancer-specific survival with utilization of univariate and multivariate analysis. Wang et al. [37] summated the results as follows:
Wang et al [37]. Made the following conclusions:
Based upon the findings and recommendation of Wang et al [37]. it would be argued that there is an urgent need for the establishment of a global multi-centre treatment trials of various aggressive treatment options for the management of primary signet-ring cell carcinomas of the urinary bladder (PSRCCUB) that would include radical cystectomy plus neoadjuvant/adjuvant combination chemotherapy, plus radical radiotherapy, plus immunotherapy in order to find a way to improve upon the survival and prognosis of patients who have primary signet-ring cell carcinoma of the urinary bladder (PSRCCUB) as well as there is need for academic urologists, academic oncologists, and academic pharmacotherapy research workers to undertake research work that would identify newer more effective chemotherapy medicaments that would safely destroy signet-ring carcinoma cells in order to improve upon the survival and prognosis of patients who have signet-ring cell carcinoma of the urinary bladder.
Grignon et al. [38] reported 12 cases of signet-ring cell carcinoma of the urinary bladder they had collected within their institution. They summarised the results of their analysis of various aspects of the tumours as follows:
The finding of Grignon et al. [38] that signet-ring cell carcinomas of the urinary bladder are aggressive tumours that are associated with aggressive biological behaviour as well as poor prognosis should be a pivot for academic urologists, oncologists, and pharmacotherapy research workers to urgently undertake research projects that are aimed at finding new treatment options that would improve the prognosis of the disease.
El Ammari [39] reported a 51-year-old Moroccan Berber man who had presented with visible haematuria. He had ultrasound scan as well as computed tomography scan which demonstrated a urinary bladder tumour which had diffusely invaded his urinary bladder wall. He underwent cystoscopy which demonstrated non-papillary sessile tumours that had occupied almost the entire wall of the urinary bladder as well as the left side of the trigone and it had also obstructed the left ureteric orifice. Incomplete trans-urethral resection of the bladder tumour was undertaken. Histopathology examination of the resected bladder tumour chips demonstrated poorly differentiated mucin-secreting adenocarcinoma of the signet-ring cell type. He underwent gastrointestinal endoscopy as well as analysis of tumour markers which did exclude an extra-vesical primary signet-ring cell tumour site. A diagnosis of primary signet-ring cell carcinoma of the urinary bladder was made. He underwent radical cystectomy plus bilateral pelvic lymphadenectomy plus ileal conduit construction. Histopathology examination of the specimen demonstrated features of an adenocarcinoma which was comprised of signet-ring cells with an abundant mucin pool which had invaded the peri-vesical adipose tissue as well as one lymph node that measured less than 2 cm for which the tumour was staged as T3bN1M0. He received adjuvant chemotherapy with 4 cycles of cisplatin, 100mg / m2 on day 1 and Gemcitabine 1000 mg/m2 on days 1 and 8 combination, every 21 days. Eighteen months pursuant to his radical cystectomy, he manifested with pelvic and back pain. He had computed tomography (CT) scan of thorax, abdomen and pelvis, which demonstrated multiple metastases within the spine, lung and pelvis. He refused to be enrolled into any additional treatment protocol and he died 4 months later because of respiratory failure. El Ammari et al. [39] concluded that the rarity and the successful treatment with carboplatin and Gemcitabine as adjuvant chemotherapy in primary signet-ring cell carcinoma which had been rarely reported within the literature are two characteristics which had been described in their reported case. Considering that despite an apparently good initial response to radical cystectomy and combination chemotherapy which was followed by the development of multiple metastases and death of the patient in less than 2 years due to the tumour, it would be argued that perhaps radical cystectomy plus adjuvant combination chemotherapy alone is not enough for the treatment of such an aggressive tumour and for this reason clinicians should consider the addition of radical radiotherapy plus immunotherapy as additional treatments to radical cystectomy and combination chemotherapy and these treatments should be commenced early.
Jin et al. [40] iterated that even though signet-ring cell carcinoma of the urinary bladder is a highly malignant tumour, it often tends to be neglected in view of the rarity of the tumour. Jin et al. [40] utilized the National Surveillance, Epidemiology, and End Results (SEER) data base (2004 – 2016) to compare signet ring cell carcinoma (SRCC) of the bladder with urothelial carcinoma (UC) of the bladder and they investigated the prognostic values of the clinicopathological features and survival outcomes in signet-ring cell carcinoma (SRCC) of the urinary bladder. Jin et al. [40] utilized Multi-variable Cox proportional hazard model, sub-group analyses, and propensity score matching (PSM). Jin et al. [40] summarized their results as follows:
Jin et al. [40] made the following conclusions:
Considering that the study of Jin et al. [40] is a recent study, it would be argued that up to date clinicians globally have not found treatment options that would drastically reduce death rates related to signet-ring cell carcinomas of the urinary bladder and for this reason it would be important for a global consensus opinion group on signet-ring cell carcinoma of the urinary bladder to be established so they can deliberate on aggressive treatment options that could improve the prognosis of the disease.
Singh et al. [41] reported a 62-year-old man who had presented with visible haematuria over the preceding 4 months. He had a CT scan of abdomen which showed an 8.0 x 2.5 cm hypoechoic solid mass within the dome of his urinary bladder which had extended into his peri-vesical fat, with no evidence of loco-regional lymph nodes, metastases, or primary tumour within the abdominal or pelvic organs. Trans-urethral resection biopsy of the urinary bladder tumour was undertaken and pathology examination of the specimen showed mucinous adenocarcinoma with signet-ring cell features. Partial cystectomy and bilateral lymph node dissection was undertaken. Macroscopy examination of the specimen demonstrated the primary tumour was covered by thick mucus. The microscopy histopathology examination features of the tumour were consistent with the diagnosis of poorly differentiated mixed mucinous and signet-ring cell adenocarcinoma with high mitotic activity of greater than 10 mitotic figures per 10 high power fields as well as areas of necrosis. The tumour was found within the lamina propria beneath an intact urothelial epithelium of the bladder with a close surgical resection margin of 1 mm to 3 mm and microscopic invasion into the peri-vesical fat. Five lymph nodes were negative. A urachal remnant could not be identified. Immunohistochemistry staining of the tumour demonstrated that the tumour cells had exhibited positive staining for CK 7, CK 20, CDX-2, E-cadherin, CEA, EMA, p53, B-catenin (nuclear stain), and Villin. The tumour cells exhibited negative staining for thrombomodulin, TTF-1, PSA and WT-1. Proliferation index (Ki-67) was light. Electron microscopy examination of the tumour demonstrated core filamentous rootlets and mucus vacuoles within the signet-ring cells. Molecular testing was negative for microsatellite instability. Upper gastrointestinal endoscopy was undertaken which was normal but colonoscopy was not undertaken. He had computed tomography scan of the abdomen and pelvis which did not demonstrate a colorectal primary tumour. Many months pursuant to his partial cystectomy procedure, he developed a fistula through an ulcerated lesion on his lip under the vermillion line which did present as pain and difficulty with eating. He had biopsy of the lower lip lesion and pathology examination of the specimen showed a tumour which had features that were similar to the features of his urinary bladder tumour. He furthermore, had computed tomography (CT) scan of abdomen which showed progressive disease within the region of the duodenal bulb, within the pancreas, anterior to his right kidney, and on both sides of his residual urinary bladder. He had an endoscopic ultrasound-scan guided fine-needle aspiration biopsy of the pancreatic mass and pathology examination of the specimen did confirm metastatic signet-ring cell carcinoma. Chemotherapy that comprised of Capecitabine 1000 mg per m2 daily for 14 days and oxaliplatin 130 mg /m2 once every 3 weeks was commenced 8 months pursuant to his partial cystectomy. He received radiotherapy to his lips at 9 months pursuant to his partial cystectomy. For the duration of his radiotherapy, oxaliplatin was withheld, but concomitant capecitabine was administered at a reduced dose. Seven (7) months pursuant to the commencement of his chemotherapy, he had radiology imaging which demonstrated stable disease within the area of the thickening on the left lateral aspect of the residual urinary bladder, as well as regression of the low attenuation areas within the right renal pelvis region, neck of the pancreas, as well as within the para-duodenal region. There was additionally almost complete resolution of the lesion on the lip and the fistula with significant improvement of his symptoms. He continued to have stable disease for 16 months before he developed progression of the tumour to his chest that became apparent. He did receive second line chemotherapy that consisted of capecitabine and irinotecan but the tumours did not respond to this treatment. He subsequently died about 24 months after the commencement of his chemotherapy. Singh et al. [41] made the ensuing concluding iterations:
Their case had raised a number of pertinent points including:
A lesson learnt from this case report is that primary signet-ring cell carcinoma of the urinary bladder is an aggressive carcinoma that is associated with poor prognosis and death of patients and in view of this when a primary signet ring-cell carcinoma of the urinary bladder is encountered it should be treated aggressive as treatment of curative intent and it could be argued that with regard to the reported case a radical cystectomy plus pelvic lymph node dissection plus combination adjuvant therapy including radical radiotherapy, combination chemotherapy plus immunotherapy should be considered an option of aggressive treatment to use rather than to wait till metastases develop.
Andreva et al. [42] reported a case of signet-ring cell carcinoma of the urinary bladder in a 26-year-old patient. Pathology examination of the urinary bladder tumour demonstrated a poorly differentiated carcinoma of the urinary bladder which was mainly signet-ring cell type with mucosal ulceration, and deep infiltrative growth which had involved the tissues around the urinary bladder. This short summation is important in that it has illustrated that signet-ring cell carcinoma which is an aggressive tumour can also affect young adults.
Matsuzaki et al. [43] reported a 59-year-old man who manifested with non-visible haematuria. He had cystoscopy which showed a white non-papillary tumour. He underwent trans-urethral resection of the tumour and pathology examination of the resected tumour demonstrated signet-ring cell carcinoma as well as transitional cell carcinoma with a histological death of invasion PT1. He did not receive any adjuvant therapy. Lessons that need to be learnt from this summation include the fact that signet-ring cell carcinoma of the urinary bladder can exist with transitional cell carcinoma and on rare occasions this rare malignant tumour could be found to be non-muscle invasive as demonstrated by invasion of the lamina propria only.
Ozeki et al. [44] reported a 58-year-old man who presented with visible haematuria and urinary urgency. He underwent cystoscopy which demonstrated multiple non-papillary broad based tumours as well as reddish unstable urinary bladder mucosa. He had trans-urethral resection biopsy of the urinary bladder tumours and pathology examination of the specimens demonstrated signet-ring cell carcinoma predominantly and adenocarcinoma transforming into signet-ring cell carcinoma partially. He underwent total cystectomy with ileal conduit urinary diversion. Histopathology examination of the cystectomy specimen showed grade 3 transitional cell carcinoma in association with adenocarcinoma. Ozeki et al. [44] were of the opinion that these findings did suggest that adenomatous metaplasia of transitional cell carcinoma within the urinary bladder could differentiate into signet-ring cell carcinoma.
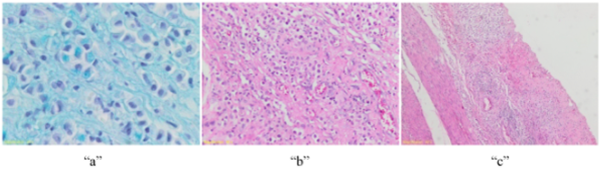
Allameh et al. [45] reported an 18-year-old Afghan male who had a past medical history of cystolithotomy seven years earlier, who had presented with a one year history of intermittent visible haematuria with amorphous blood clots. He had ultrasound scan of renal tract and abdomen which showed non-uniform decrease in the parenchyma of both kidneys as well as bilateral hydronephrosis which was dominant in the left side (Grade III) as well as partial defect on the left urinary bladder wall. He had contrast-enhanced computed tomography (CT) scan which showed bilateral hydronephrosis which was dominant on the left side; non-uniform decrease in the cortex of both kidneys as well as multiple filling defects were demonstrated within the lumen of the urinary bladder without evidence of distant metastasis (see figure 5). He underwent trans-urethral resection of urinary bladder tumour which on gross visualization was noted to be a white, calcified, sessile tumour which had extended from the left side of the urinary bladder wall to the dome and the tumour had obstructed his left ureteric orifice. Trans-urethral resection of the bladder tumour (TURBT) was undertaken and left nephrostomy insertion was undertaken. The specimens was sent for polymerase chain reaction for assessment to evaluate for tuberculosis, in view of the fact that tuberculosis, is widespread in Afghanistan, Diffuse urethral stricture, non-papillary mass, as well as diffuse erythema results were all negative. Histopathology examination of the specimen showed features that were consistent with poorly differentiated mixed mucinous and signet-ring cell adenocarcinoma. Immunohistochemistry staining studies of the tumour demonstrated that the tumour cells had exhibited strong positive staining for CK7, CK 20, and CDX-2, as well as the tumour cells had exhibited negative staining for PSA, CK34ßE12, as well as for Vimentin. The provisional differential diagnoses included (a) primary urinary bladder adenocarcinoma and (b) metastatic adenocarcinoma from a tumour which primarily originated from the gastrointestinal tract. He underwent esophagogastroduodenoscopy and recto-sigmoidoscopy which were normal. He also had normal tumour marker levels of CA 19-9, and CA 125 which excluded possible extra-vesical primary lesions. He also had trans-rectal biopsies of the prostate gland and pathology examination of the specimens were normal in that no malignant lesion was found in the samples of the prostate gland. He underwent radical cystectomy plus prostatectomy sparing the seminal vesicle and prostate preservation and orthotopic urinary diversion with “W” ileum pouch plus pelvic lymphadenectomy to the bifurcation of the aorta and bilateral ureteric stents were inserted. Gross examination of the cystectomy specimen demonstrated an ill-defined ulcerative as well as necrotic tumour mass that had soft as well as gelatinous consistency that filled the cavity of the entire urinary bladder wall that measured 2.5 cm with regard to its maximum thickness. Microscopic examination of the tumour showed that the urinary bladder wall was infiltrated into deep muscularis propria by a necrotic tumour which comprised of lakes of mucins that contained floating nests or cords of epithelioid cells as well as many signet-ring cells (see figure 6(a) and figure 6(b). Microscopy examination of the specimen did not demonstrate any remnant of the urachus. A final diagnosis of signet-ring variant of mucinous adenocarcinoma of the urinary bladder was established. No metastatic lymph node was identified so the tumour was staged T2N0M0 signet-ring cell carcinoma of the urinary bladder of the mucinous adenocarcinoma variant. At his six months post-operative follow-up assessment, the results of his clinical examination, chest X-rays, computed tomography (CT) scans and cystoscopy were all normal which had indicated there was no local recurrence of tumour or distant metastasis.
A lesson that has been learnt from this case report is the fact that primary signet-ring cell carcinoma can also affect the younger the age group including teenagers and clinicians need to have a high index of suspicion for such a rare and aggressive tumour. Considering that primary signet-ring cell carcinoma of the urinary bladder is a very aggressive tumour, it would be argued that the option of radical cystectomy plus combination adjuvant therapies including chemotherapy, radiotherapy as well as immunotherapy should be considered as treatment options to provide treatment of curative intent.
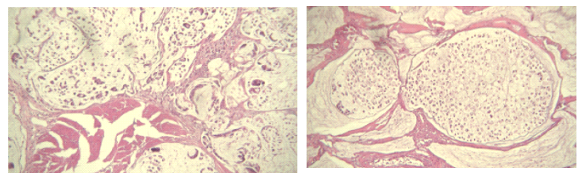
Armache et al. [46] reported a 66-year-old man who presented with painless visible haematuria over the preceding one month. He had ultrasound scan of the pelvis which demonstrated a thickening of the wall of his urinary bladder. He had a computed tomography (CT) scan of abdomen and pelvis which did not show any obvious urinary bladder mass or distant metastases; however, only a diffuse thickening of the urinary bladder wall associated with bilateral enlargement of the inguinal and iliac lymph nodes (see figure 7). He had cystoscopy which demonstrated multiple sessile tumours within his left bladder wall, base and dome of the bladder. He underwent trans-urethral resection of the bladder tumour. Histopathology examination of specimens of the resected bladder tumour demonstrated features that were consisten with the diagnosis of a signet-ring cell carcinoma of the urinary bladder sub-type of adenocarcinoma that had infiltrated the lamina propria and muscularis (stage pT2). He underwent gastroduodenoscopy and colonoscopy as well as his CEA tumour marker levels were determined and all these investigations were normal and had excluded a primary tumour site within the gastrointestinal tract. Based upon the results of the investigations, a diagnosis of primary signet-ring cell carcinoma of the urinary bladder was made. He underwent radical cystoprostatectomy with an ileal conduit and bilateral pelvic lymph adenectomy. A frozen pelvis was found during the operation. Pathology examination of the radical cystectomy specimen revealed features of a poorly diffrentiated adenocarcinoma of the urinary bladder which had comprised of signet-ring cells that contained an abundant mucin pool with invasion of the peri-veical fat (see figure 8). The right ureteral margin was free of tumour even though the left ureteric margin was initially focally reached by the tumour. The histopathology staging of the tumour was pT3bN1M0. Immunohistochemistry staining studies of the tumour did show that the tumour cells had exhibited positive staining for Cytokeratin 7, CEA, and CA 19-9 and the tumour cells exhibited negative staining for CD-X2 (see figure 9). He received six cycles of adjuvant chemotherapy that consisted of carboplatin and Gemcitabine cobination, but he died six month later from a heart attack.


Hirano et al. [47] reported a 65-year-old man who had presented with visible haematuria in November 1997. He had ultrasound scan of renal tract which showed left hydronephrosis. He had intravenous urography which demonstrated a non-functioning left kidney as well as a filling defect on his left bladder wall. He had computed tomography (CT) scan and magnetic resonance imaging (MRI) scan which showed left hydronephrosis and an invasive urinary bladder tumour but no evidence of distant metastasis. He underwent cystoscopy which showed a white, sessile tumour which had extended from the left wall of his urinary bladder to the trigone and which had obstructed the left ureteric orifice. Punch biopsy and trans-urethral resection of the tumour were undertaken. Histopathology examination of the specimens demonstrated that the tumour cells had formed abundant mucin and positive staining of cytoplasm by Periodic acid Schiff. A component of the tumour was noted to be high-grade transitional cell carcinoma. He underwent esophagogastroduodenoscopy and recto-sigmoidoscopy which did not demonstrate any tumour and had excluded a primary tumour from the gastrointestinal tract. A diagnosis of primary signet-ring cell carcinoma (PSRCC) of the urinary bladder T3BN0M0 was established. It was recommended that the patient should undergo radical cystectomy but the patient refused to undergo radical cystectomy. He received intra-arterial chemotherapy with utilization of Carboplatin. Angiography catheter was inserted via his left femoral artery into the left internal iliac artery near the branch of the vesical artery with utilization of Seldinger technique. The left superior gluteal artery was embolized to prevent necrosis of the hip by the carboplatin. 400 mg of Carboplatin was instilled via the left catheter. Thereafter, 200 mg of Carboplatin was instilled into the right vesical artery. Three courses of intra-arterial infusion of carboplatin were undertaken at 3 weeks intervals. One month pursuant to the completion of the treatment, he had computed tomography (CT) and magnetic resonance imaging (MRI) scans as well as cystoscopy and biopsy of the bladder which all demonstrated features that confirmed complete disappearance of the cancer. At the time of publication of the article the patient has had complete remission that had been maintained for 44 months with no evidence of local recurrence or metastasis.
Tagami et al. [48] iterated that primary signet-ring cell carcinoma of the urinary bladder is an uncommon tumour which has tended to be associated with poor prognosis. Tagami et al. [48] stated that there are few successful chemotherapy treatments for this tumour. Tagami et al. [48] reported a case of chemotherapy with a docetaxel regimen which did prove to be efficacious in a 64-year-old Japanese, who was suffering from signet-ring cell carcinoma of the urinary bladder. Tagami et al. [48] reported that the onset of bilateral hydronephrosis did lead to the detection of the urinary bladder tumour and pathology examination of the tumour showed features of signet-ring cell carcinoma of the urinary bladder. Immunohistochemistry staining studies of the tumour showed that the tumour cells had exhibited positive staining for cytokeratin 7 +, and cytokeratin 20+/-. In view of the fact that the tumour had invaded the patient’s abdominal wall and groin he could not be offered surgery but instead he was treated with utilization of chemotherapy. The patient initially received 2 courses of chemotherapy which did comprise of S-1 and cisplatin; nevertheless, this treatment was not effective. Tagami et al. [48] chose docetaxel as a second-line chemotherapy regimen which comprised of 60 mg / m2, tri-weekly, and his follow-up clinical examination and contrast-enhanced computed tomography demonstrated that his disease had successfully responded to the chemotherapy. Some lessons that can be learnt from this case summation include the following:
Conflict of interest – None
Acknowledgements to:
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
